
Forced to suffer for science: From animal cruelty and experimental inefficiency to a change of perspective.
We, as scientists, have become desensitised to the pain, the distress and the physical and emotional damage that we inflict on laboratory animals. So much so, that we constantly find justifications for our cruel experiments in the goal of finding cures for the illnesses of our conspecifics, and in the rules and regulations that authorise these heartless procedures.
Despite ongoing widespread use of animal models in research, recently there has been extensive criticism on the state of drug development in psychiatry, calling for a switch from rodent behavioral pharmacology to mechanistic studies in cellular systems. In a recent paper, Heilig and colleagues argue that:
Overall, neuroscience has simply had very little impact on clinical alcoholism treatment. The situation is representative of a broader translational crisis in psychiatric neuroscience. Because translational failures in this area have been the rule rather than the exception, pharmaceutical industry has largely retracted from efforts to develop novel psychiatric medication. As a result, the utility of animal models in research on psychiatric disorders, including addiction, is also being questioned.
Heilig et al. (2019)
Caricature Cruelty
Several experimental paradigms employed by labs all over the world, for elucidating the mechanisms of mental disorders and for the development of new psychiatric drugs, consist of procedures that innevitably cause suffering to the experimental animals. From learned helplessness paradigms (forced swim and tail suspension), intended to model the symptoms of depression in humans, to neuropathic pain models, which involve nerve operations to induce chronic pain in rats or mice, as well as fear conditioning experiments, consisting of series of electric shocks on consecutive days, large numbers of laboratory animals across the globe are subjected to procedures at the end of which they are euthanized for histological analyses.
The two videos below illustrate two paradigms for learned helplessness in rodents – forced swim and tail suspension, respectively. Even for those unfamiliar with these methods, it is not hard to notice the amount of distress and fear the animals are forced to go through.


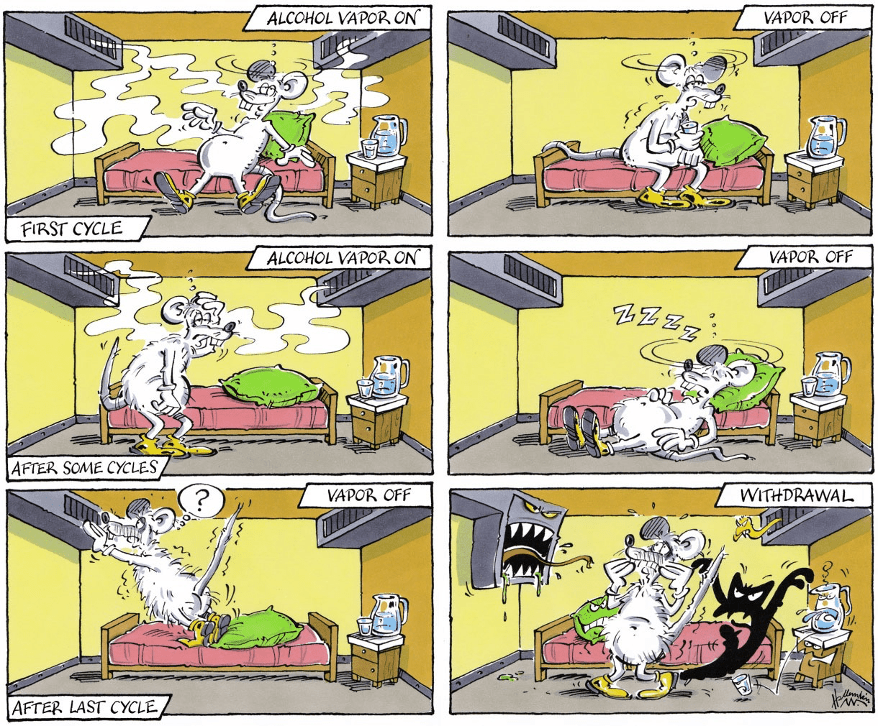
Another example, otherwise claimed to be minimally invasive and highly relevant for medication testing (Meinhardt and Sommer, 2015), is the post-dependent animal model, a model for medication development in alcoholism. It involves inducing dependence through repeated intermittent cycles of alcohol vapour exposure. In other words, rodents (usually, rats) are exposed every day, for several weeks or months, to cycles of intoxication with alcohol vapours, alternating with withdrawal, which ultimately result in compulsive alcohol intake, excessive alcohol seeking, hypersensitivity to stress as well as the development of an alcohol withdrawal syndrome, which better resemble human alcoholism.
Rats usually undergo 5 cycles of 14 (sometimes, 16) hours of forced exposure to alcohol vapours, separated by 10-hour periods of withdrawal and an additional 58 hours at the end of each weekly cycle. These cycles take place over many weeks. As a result of severe alcohol intoxication, some rats die during the experiment. At the end of the last alcohol exposure, the rats that have survived are decapitated.
The sardonically humorous caricatures below, selected from (Meinhardt and Sommer, 2015), not only illustrate the procedure, but are at the same time indicative of a certain emotional detachement these scientists have developed from the rats they used in their experiments.

“Unavoidable” Suffering
Granted, there have been attempts at reducing the suffering of these poor animals. The three Rs – Replacement, Reduction and Refinement – reflect the scope to encourage alternatives to animal testing, as well as improving animal welfare in experiments where the use of animals is unavoidable. The 3Rs have been incorporated into the legislation governing animal use in many countries, in order to ensure that the use of animals in testing is as ethical as possible.
And yet, with paradigms such as forced swimming test, also known as the behavioural despair test, or the tail suspension test ( where the rodent is hanging from its tail upside down and is unable to touch the walls of the compartment), it is clear that there is a big discrepancy between what could be done and what is actually being done. We could move away from these cruel practices, which have been demonstrated to be misleading and offer little understanding on the mechanisms behind psychiatric conditions, and, instead, resort to alternative strategies, which have the potential to set research on a path of true breakthroughs in psychiatry (as it is being presented in a later section). However, most papers focused on schizophrenia, anxiety, depression, Alzheimer’s disease, addiction etc. rely on experiments which would make the skin of the more sensitive of us crawl, and those with a tougher skin reconsider their academic career (such as switching to cognitive neuroscience and human-based studies only, in my case).
It is also important to remember that, not only the procedures themselves cause pain and suffering to the experimental animals, but often times the side-effects of the medications being tested on them and the behavioral tests they are being used in result in long-term health consequences – for instance, postdependent alcoholic rats end up developing peripheral secondary osteoporosis.
When suffering exceeds a certain limit, the animals are usually euthanized. What a great life these creatures must have, given that one of the best solutions to end their pain is premature death…
Rats empathise with other helpless rats
Although we all know that “animals have feelings too”, we are still far from understanding to what extent animals actually feel. In humans, for instance, pain and consciousness are tightly linked. We do not yet know which animals have consciousness and what (if anything) that consciousness might be like.
That being said, a study from 2011 demonstrated that rats exhibit emotional responses and empathy. In their experiment, Bartal and colleagues showed that when a free rat occasionally heard distress calls from another rat trapped in a cage, it learned to open the cage and released the other animal even in the absence of a payoff reunion with it. The free rat would even save a chocolate chip for the captive.

The presence of a rat trapped in a restrainer elicits focused activity from his cagemate, leading eventually to door-opening and consequent liberation of the trapped rat. (Science/AAAS).
This experiment clearly shows that rats, and possibly other animals as well, are capable of complex emotional experiences, previously only attributed to humans (more studies should be done to investigate this fascinating and important topic). Alas, in the absence of a deep understanding of the animal psyche, and moreover, with clear indications that animals possess the capacity to feel almost to the same extent as us humans do, we still continue to abuse them in our cruel experiments.
The issues with animal models
Valid disease models do not exist for psychiatric disorders.
Hyman (2012)
On the rodent models based on learned helplessness, Hyman went on to argue that:
Forced-swim and tail suspension tests do not even model the therapeutic action of antidepressants, because in those rodent screens a single dose of antidepressant is active, whereas in dependent patients, antidepressant drugs require weeks of administration to exert a therapeutic effect.
Hyman (2012)
In fact, given that most psychiatric diseases are heterogenous and polygenic, often times animal behavioral models have turned out to be misleading. Shockingly, only 8% of the CNS drug candidates developed between 1993 and 2004, which reached initial human testing, were approved to be used as medication. The main drawbacks of these drugs were the toxicity discovered in late-stage clinical trials, along with the inability to demonstrate efficacy. Not to mention the serious side effects these drugs produce in humans, such as weight gain and metabolic derrangements.
Animal models, albeit useful for some translational investigations and for basic studies in neuroscience, present various limitations:
- Lack of molecular and neural circuit-based characteristics, which are required for molecular studies of psychiatric diseases.
- The construction of transgenic mice is too slow and expensive.
- Regarding non-human primates, the challenges involve cost, less well-developed technologies as well as ethical barriers.
- When it comes to invertebrate models or zebrafish (extensively used in translational research), evolutionary distance poses huge obstacles in translational psychiatry, although they could be useful in the initial molecular investigations of the functions of risk alleles emerging from genetic studies.
Given the above-mentioned drawbacks of relying on animal models to develop psychiatric treatments, major pharmaceutical companies have already decided to move away from these old-fashioned approaches. Now, the question remains, what is there to do in the future?
Adopting new strategies in psychiatric research
Science needs to move forward and find better methods to study the highly complex mechanisms underlying psychiatric diseases, in order to allow for truly efficient drugs and therapies to be developed. As mentioned earlier, animal-based studies have more often than not failed to identify pharmaceutical compounds with positive outcomes in humans.
Over the last half-century, despite the identification of several antipsychotic and antidepressant drugs, alongside the discovery of various neurotransmitters, receptors and transporters involved in mental illnesses, objective diagnostic scans are scarce, and, surprisingly, only a handful of validated molecular targets have been established.
Luckily for us, there are several alternative solutions, which are already being seriously considered by various laboratories and drug companies, as listed below:
- DNA sequencing, which is nowadays much cheaper than it used to be (by 1 million-fold), makes it possible to analyse large number of subjects, in the attempt to identify genes involved in the heterogenous, polygenic psychiatric disorders.
- Large scale studies of gene function, epigenetics, transcriptomics and proteomics would contribute to the understanding of pathogenesis.
- Optogenetics, a technology with increasing popularity in neurobiology, allows researchers to activate or inhibit single cell types, thus detecting which circuits are specific to certain disorders.
- Human neurones derived directly from skin fibroblasts and blood cells in vitro, or generated from human embryonic stem cells (hESCs) or induced pluripotent stem cells (iPSCs) in vitro.
- These above-mentioned tools can be combined with electrophysiological and neuroimaging data from humans, which can indirectly reveal abnormal functioning of widely distributed circuits.
What psychiatric research needs is to be able to accurately model molecular mechanisms of disease, instead of relying on behavioral results. Since I already mentioned large-scale genetic as well as epigenetic strategies, it is fair to admit that such studies require suitable living systems in which experiments can be conducted (given that the living human brain is not accessible, and that postmortem studies have limitations when it comes to functional analyses). Although, in some circumstances, animal behavioral experiments can help in elucidating treatment options, conclusions ought not to be based on modelling disease symptoms, as these can be misleading and often fail to translate into human psychopathology. Moreover, symptoms change over time and depending on the context, and are based on subjective rating scales, making the comparison between human and animal conditions difficult.
The solution is plain and simple – scientists and pharmaceutical companies must, first of all, unanimously and once and for all come to terms with the fact that the efforts based on cruel animal studies have been of too little avail to justify their continuation. Instead, a new strategy must be incorporated by the scientific community in psychiatric research, which should carry on from cell-based models and established molecular mechanisms to early human trials, skipping the intermediate step of animal behavioral models.
To end on a cheerful note, here is a heartwarming video which proves there is hope that the future could look bright for laboratory animals if people are willing to start making a change:

Special thanks to my mom for insightful comments and for her constant support, and to Gasser Elmissiery for inspiring discussions and for his contribution to creating the featured image.
References
- Bartal, I. B.-A., Decety, J., & Mason, P. (2011). Empathy and Pro-Social Behavior in Rats. Science, 334(6061), 1427 LP – 1430. doi:org/10.1126/science.1210789
- Haaranen M, Scuppa G, Tambalo S, Järvi V, Bertozzi SM, Armirotti A, Sommer WH, Bifone A, Hyytiä P. (2020). Anterior insula stimulation suppresses appetitive behavior while inducing forebrain activation in alcohol-preferring rats. Transl Psychiatry. 10(1):150. doi: 10.1038/s41398-020-0833-7
- Hansson AC, Koopmann A, Uhrig S, Bühler S, Domi E, Kiessling E, Ciccocioppo R, Froemke RC, Grinevich V, Kiefer F, Sommer WH, Vollstädt-Klein S, Spanagel R. (2018). Oxytocin Reduces Alcohol Cue-Reactivity in Alcohol-Dependent Rats and Humans. Neuropsychopharmacology. 43(6):1235-1246. doi: 10.1038/npp.2017.257
- Heilig M, Augier E, Pfarr S, Sommer WH. (2019). Developing neuroscience-based treatments for alcohol addiction: A matter of choice? Transl Psychiatry. 9(1):255. doi: 10.1038/s41398-019-0591-6
- Hyman SE. (2012). Revolution stalled. Sci Transl Med. 4:155cm11
- Knobloch HS, Charlet A, Hoffmann LC, Eliava M, Khrulev S, Cetin AH, Osten P, Schwarz MK, Seeburg PH, Stoop R, Grinevich V. (2012). Evoked axonal oxytocin release in the central amygdala attenuates fear response. Neuron. 73(3):553-66. doi: 10.1016/j.neuron.2011.11.030
- Meinhardt MW, Sommer WH. Postdependent state in rats as a model for medication development in alcoholism (2015). Addict Biol. 20(1):1-21. doi: 10.1111/adb.12187
- Wahis, J., Kerspern, D., Althammer, F., Baudon, A., Goyon, S., Hagiwara, D., … Charlet, A. (2020). Oxytocin Acts on Astrocytes in the Central Amygdala to Promote a Positive Emotional State. BioRxiv, 2020.02.25.963884. doi:org/10.1101/2020.02.25.963884



