
The biological implications of meditation practices in the treatment of depression
Major depressive disorder (MDD) is a common mood disorder and a great cause of disability worldwide. Biological factors implicated in MDD range from neural imbalances to signaling dysregulations (which are partly grounded in genetic predispositions).
As shown in Figure 1, the socio-cognitive and biological deficiencies involved in MDD appear to influence each other in a circular, perpetuating manner. These deficiencies can be categorized into six non-exhaustive broad factors, i.e., mood, executive functioning, social skills, neuroplasticity, neural core networks, and neuroendocrine and neuroimmunological factors. The modulation of one factor is expected to exert an effect over the other factors, and subsequently to affect the overall depressive symptomology. Importantly, although these factors seem to play a causal role in the symptoms of MDD to various degrees, the precise causes of depression have not yet been entirely determined. There are, for instance, other psychological (e.g. cognitive biases) and biological factors (e.g. serotonin transporter genotype) that are known to be involved in depression, however these will not be covered in this article.

Particularly impaired in individuals with MDD is neuroplasticity, a crucial neural mechanism that entails structural and functional brain adaptations in response to altered environmental circumstances. This impairment is generally indicated by abnormally low levels of the brain-derived neurotrophic factor (BDNF), which is related to hippocampal and prefrontal atrophy in MDD. Moreover, impairments in stress regulation and immune system functioning have also been associated with the development of MDD symptoms. The following paragraphs describe in more detail the roles of BDNF, as well as those of cortisol, as a marker of stress, and of inflammatory cytokines in mental health, with a focus on depression.
BDNF is an important neurotrophin which promotes neuronal development, survival and plasticity in the central and peripheral nervous systems. It is most active in brain areas that play a role in learning, memory and higher cognition, such as the hippocampus and cortex. BDNF is also pivotal in the regulation of several physiological aspects, including stress response, mood, inflammation and metabolism. Decreases in BDNF levels have been linked to psychiatric and neurological disorders, such as depression, anxiety and Alzheimer’s disease.
Cortisol is a glucocorticoid secreted by the adrenal glands and, as part of the hypothalamic-adrenal-pituitary (HPA) axis, is a reliable marker for stress response. Cortisol is also part of the feedback mechanism in the immune system, where its role is to reduce certain aspects of the immune function, such as inflammation. Moreover, this hormone follows a robust circadian rhythm, which peaks 30 min after awakening, termed the Cortisol Awakening Response—CAR, and gradually declines throughout the day.
The circulating pro-inflammatory cytokines Interferon Gamma (IFN-γ), Interleukin-1β (IL-1β), Interleukin-6 (IL-6), Interleukin-8 (IL-8), Interleukin-12 (IL-12) and Tumor Necrosis Factor (TNF-α), as well as the anti-inflammatory cytokine Interleukin-10 (IL-10) have been extensively investigated over the past 20 years for their roles in depression, anxiety and various other chronic medical illnesses. Typically, decreases in inflammatory pathway activation during periods without active infection are associated with better physical and mental well-being. That being said, a general decrease in pro-inflammatory (and increase in anti-inflammatory) immune mediators is not necessarily indicative of health and wellness, since acute inflammatory responses are known to be adaptive; instead, a healthy homeostatic balance between pro- and anti-inflammatory signaling is most beneficial. Moreover, chronic inflammatory states can be triggered through psychosocial stress.
The deficits within these factors result in profound impairments in daily functioning, reduced quality of life, an increased risk of suicide, and a substantial lack of productivity. It is clear that there is a dire need to come up with alternative treatments for depression, next to the conventional first-line psycho- and pharmaco-therapies. One such alternative therapeutic strategy is meditation.
How meditation can alleviate the symptoms of depression ~ a biological standpoint
Mindfulness meditation is already being used in certain mental health facilities under different forms of psychotherapeutic intervensions, such as mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT). These usually consist of sessions guided by a professional in addition to at-home practice, over a duration of several weeks. While MBSR is tailored to the management of stressful situations, MBCT involves strategies for dealing with maladaptive thought patterns, which makes it more suitable for the prevention of depressive relapse. Upon repeated training, mindfulness meditation can lead to relatively global cognition-enhancing effects, as shown in Figure 2.
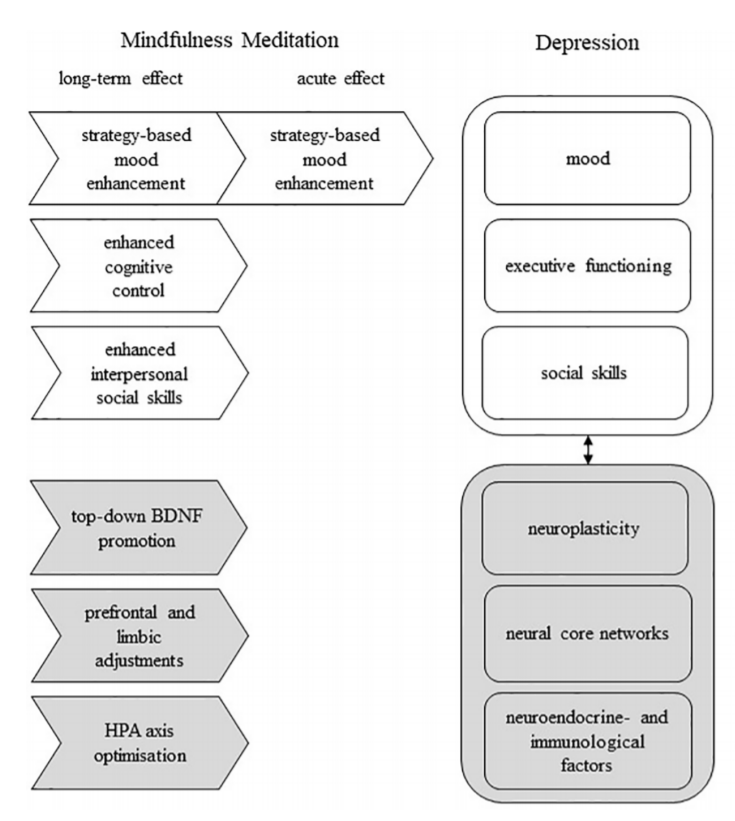
Adapted from Heuschkel and Kuypers (2020)
Meditative practices based on stress-reduction mechanisms and psychophysiological self-regulation are associated with anti-inflammatory benefits, through their modulation of inflammatory and HPA axis activities. In a study by Cahn et al. (2017), thirty-eight individuals participated in a 3-month yoga and meditation retreat, and were assessed before and after the intervention for psychometric measures, BDNF levels, circadian salivary cortisol levels, and pro- and anti-inflammatory cytokines. Participation in this yoga and meditation retreat was associated with better coping with stress, also known as stress resilience, as well as decreased self-reported depression, increased mindfulness, and generally enhanced well-being. The plasma levels of BDNF were increased by three fold post-retreat compared to pre-retreat, and this increase was inversely correlated with participants’ self-reported anxiety levels on a questionnaire (the Brief Symptom Inventory-18, BSI-18). In addition, the CAR levels were also significantly higher in these participants after the retreat, indicating improvements in the dynamic rhythmicity of the HPA axis activity, which is a marker of better stress resilience.
The researchers also found an unusual pattern of increases in both anti-inflammatory IL-10 as well as pro-inflammatory TNF-α, IFN-γ, IL-1β, IL-6, IL-8, with simultaneous decreases in the pro-inflammatory IL-12. While overall there are inconsistencies across studies on the influence of meditative practices on the immune system, it is also important to bear in mind that these studies tend to differ with respect to the type of intervention (e.g., Kundalini yoga vs. MBSR vs. Tai Chi), population (e.g., clinical vs. non-clinical), setting, design and other methodological factors; these differences lead to complexities involved in interpreting cytokine and other biomarker samples.
Having said that, pro- and anti-inflammatory response modulations may be adaptive depending on the context, for instance in chronically inflamed body states versus non-inflamed healthy normals. It is likely that in relatively healthy adults, intense yogic and meditative practices recruit an integrate brain-body response, resulting in enhanced pro- and anti-inflammatory signaling processes, which on the one hand support an upregulated vigorous immunological surveillance system, while on the other hand concomitantly promote high expression of the anti-inflammatory ‘‘break’’ such as IL-10.
Overall, the biological findings in the above-mentioned study correlate with enhanced stress resilience and well-being. At the end of an intensive three-month yoga-meditation retreat, the increased BDNF signaling and increased CAR were likely related to improved neurogenesis and/or neuroplasticity, and to enhanced alertness and readiness for mind-body engagement, respectively, while the higher levels of anti- and pro-inflammatory cytokines suggested better immunological readiness. Further research should attempt to investigate the role of other contextual factors (e.g., social dynamics, diet, natural environment, relative impact of a revered spiritual teacher etc.) impacting the expression and regulation of these biological processes.
To conclude, it is evident that meditation exerts beneficial effects on the brain. Particularly important to mental disorders, when meditation is used as a therapeutic intervention, it contributes to improving mental states and cognitive abilities by influencing several key biological factors crucial for normal brain functioning.
References
- Cahn, B.R., Goodman, M.S., Peterson, C.T., Maturi, R., Mills, P.J. (2017). Yoga, Meditation and Mind-Body Health: Increased BDNF, Cortisol Awakening Response, and Altered Inflammatory Marker Expression after a 3-Month Yoga and Meditation Retreat. Front Hum Neurosci, 11:315. doi: 10.3389/fnhum.2017.00315
- Dutta, A., McKie, S., Downey, D. et al. (2019). Regional default mode network connectivity in major depressive disorder: modulation by acute intravenous citalopram. Transl Psychiatry 9, 116. doi: org/10.1038/s41398-019-0447-0
- Heuschkel, K., & Kuypers, K.P.C. (2020). Depression, Mindfulness, and Psilocybin: Possible Complementary Effects of Mindfulness Meditation and Psilocybin in the Treatment of Depression. A Review. Front. Psychiatry, 11:224. doi: 10.3389/fpsyt.2020.00224
- Zeidan, F., Johnson, S., Diamond, B., David, Z., & Goolkasian, P. (2010). Mindfulness meditation improves cognition: Evidence of brief mental training. Consciousness and Cognition, 19, 597-605. doi: org/10.1016/j.concog.2010.03.014





