
Neuroscience
‘Gather’ for poster presentation at the German Neuroscience Conference
Recently, I have had the pleasure to experience the ‘Gather’ platform, where several posters including my own were presented, as part of the 14th Göttingen Meeting of the German Neuroscience Conference. The platform is really fun to navigate and a great way to interact with fellow presenters and interested participants. I took a short video while I was navigating through the rooms.
As for my poster, I will soon upload it on the blog 🙂


On the nature of pain
Last week, a manatee was found in Florida waters, with the word ‘Trump’ scraped on its back. Although this kind of ruthless mutilation is horrific in itself, I started wondering if the animal felt any kind of pain.
I must admit, up until I came across the news about what happened to the manatee in Florida, I knew very little about manatees, in general. And my first thought was whether, during the scraping proccess, this manatee suffered at all. To my dismay, there were not many scientific papers dealing with the somatosensory system in manatees. However, I did find something that eased my soul a little bit: one of the articles reporting on the dreadful event states that the scratch was done in the algae growing on the animal’s back. Still, in the same article it is said that manatees have sensory hairs and nerves in their skin, which means that, if the cuts had touched the skin, they could have caused pain; not to mention the infection that the skin was at risk of, due to the open wounds.
The video below shows the above-mentioned manatee swimming, with the human-made scars on its back.
After reading all these news articles, I was left with some questions that kept occupying my mind: What are manatees?; To what extent can they feel pain?; And can we talk about ‘pain’ at all in manatees, or just nociception? Lastly, how did pain evolve throughout the animal kingdom?
What are mantees?
Also known as ‘sea cows’, manatees (Trichechus manatus latirostris) are herbivorous acquatic mammals of the Order Sirenia. As the name of their order suggests, manatees are believed to be the animals behind the myths of mermaids. For those interested in how manatees inspired mermaid legends, please check out the video below.
Manatees are the largest vegetarian animal to inhabit the sea, and they communicate with each other through high-pitched sounds. They are also very gentle and lack defense mechanisms, given that they do not have any natural enemies. However, they have become and endangered species, due to human activity, which is the manatee’s greatest threat. According to the Florida Fish and Wildlife Conservation Commission, the year 2020 was a hard one for manetees as well: 637 of them died, 90 of which were victims of boat collisions, and another 15 were killed by other interactions with humans.
Although manatees do not possess a highly acute visual system, they compensate for that by the presence of tactile hairs, or vibrissae, spread all over their body, especially on the face. This distribution of vibrissae is something unique among mammals, and to manatees it is highly useful in allowing them to navigate in the water.
Since mantees rely tremendously on tactile inputs, it comes as no surprise that their brains are organised to support somatosensation. The primary somatosensory cortex of manatees occupies 25% of their neocortex. Moreover, the sixth layer of their cortex contains clusters of neurons, known as Rindenkerne, which are believed to process information related to the manatee’s facial and bodily vibrissae. Although the Rindenkerne cells of manatees are somewhat similar to other cortical representations of vibrissae, termed ‘barrels’, in rodents, shrews, opposums and hedgehogs, Rindenkerne are unique to sirenia. These neuronal aggregates become active when manatees engage in tactile exploration and object recognition.
At the subcortical level, manatees possess three types of somatosenroy nuclei in their brainstems, namely the Birchoff’s nucleus, which receives information from flukes, the cuneate-gracile nucleus, which processes inputs from flippers and body trunk, and the trigeminal nucleus, which receives sensory inputs from facial vibrissae. Figure 1. below shows the somatosentory representations of the manatee’s body parts, in a coronal section of the brainstem. The thalamus also has specialised somatosensory nuclei, which differ in size, depending on their functional relevance to somatic sensation.


Figure 1. Left diagram based on image by Isuru Pryiaranga. Right image from Sarko et al. (2007), showing functional divisions withing the brainstem, corresponding to the manetee’s body parts.
Given that somatosensation is so developed in manatees, one burning question is whether they feel pain.
What is pain?
Pain is different from nociception. However, pain from injury cannot occur without nociception. The latter reffers to the process of detecting injury by the activation of a special class of receptors found in the skin, as well as deep tissues and organs, known as nociceptors. The detection of potentially or actually damaging stimuli is followed by a reflex withdrawal reaction, or nociceptive behaviour, mediated by nerves in the spinal cord. The nerve fibres that detect noxious stimuli are Aδ fibres and C fibres, which have their cell bodies in the dorsal root ganglion (DRG) of the spinal cord, as shown in Figure 2.
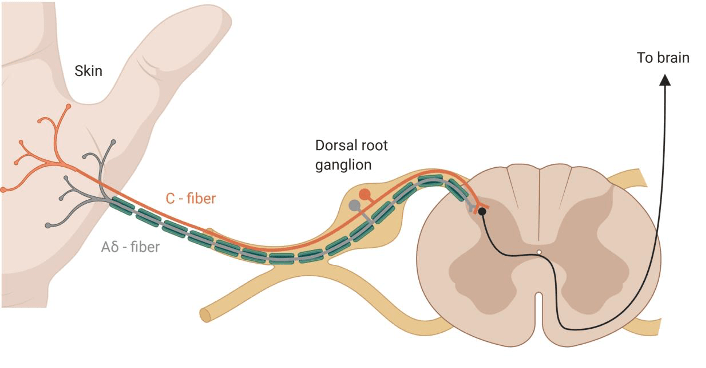
Aδ fibres are mechano-nociceptors, meaning that they are activated by high mechanical pressures. C fibres are polymodal, which means that they respond to a variety of noxious stimulations, such as noxious chemicals (e.g., acids), extreme temperatures and high mechanical pressures. They not only encode the stimulus modality (type), but also their intensity and duration, which are relayed to reflex centres in the central nervous sytem, mediating withdrawal reactions.
The nociceptive information travels from the DRG to different parts of the brain via spinothalamic tracts (from the spinal cord to the thalamus) and sensory fibres of the trigeminal tract (from the face to the thalamus). And it is within the brain that pain happens.
Pain is a complex feeling. Many brain areas are involved in not just generating pain, but also in ameliorating it. Structures from the limbic system, such as the amygdala, receive and integrate nociceptive and affect-related information. The amygdala can lead to increased nocifensive and affective pain behavior, while, under certain circumstances, it can also contribute to endogenous pain inhibition. Pain is also processed in the hypothalamus, the basal ganglia, the insula and the somatosensory cortices. Because these areas play a role in metabolism, as well as fear, pleasure and homeostasis, the nociceptive information is integrated and modulated according to the current state of the individual. In some situations, pain becomes pathological, as it is the case in neuropathic pain, where either previously innocuous stimuli become painful (aka, allodynia), or previously painful stimuli become even more painful (aka, hyperalgesia).
There are two brainstem structures, which are highly involved in controlling pain and generating analgesia. One of them is the periaqueductal grey (PAG) and the other is the rostral ventromedial medulla. These regions exert control over pain to prioritise competing stimuli, and to maintain homeostasis and survival. You might have noticed that, in highly stressful situations you do not feel pain. This is known as stress-induced analgesia, a phenomenon whereby the brain responds to stress by the production of endogenous opioids that act as natural analgesics in the nervous system. The opioid receptors found in the brain are the same ones which analgesic drugs, such as synthetic opioids and morphine, act on to relieve pain.
The evolution of pain
Many animal taxa have nociceptors. A schematic of the evolutionary development of nociceptors and the types of noxious stimuli they respond to is presented in Figure 3. In order to process nociceptive inputs, animals need a central nervous system (spinal cord and brain). It might come as a surprise that such a system, though at different levels of complexity, is found in all kinds of animals, including insects (like Drosophila melanogaster, the fruit fly), C. elegans (a type of worm highly studied in neurosciences), fish, amphibians, reptiles, birds and, of course, mammals.

Taken from Sneddon (2017)
Life-history shapes pain perception. A very interesting example is the African naked mole rat, which lives in underground burrows that are poorly ventilated, hence contain high carbon dioxide levels. As a result, the C fibres of the naked mole rat are unresponsive to acid, which means that, while other mammals find acidic environments nociceptive, the African naked mole rat does not.
When it comes to acquatic animals, such as manatees, they are expected to have differences in their sensory system compared to terrestrial ones, due to distinct ecological and evolutionary pressures. In water, any chemicals become dilluted, shifts in temperatures are less common, and there is no mechanical damage due to falling. Thus, acquatic animals are possibly at a lower risk of damage than terrestrial animals, which has implications on their nociceptive system.
As far as manatees go, it is still unclear to what extent they feel pain. The fact that they are an endangered species makes is difficult to study them. But given that they posses a very well-developed somatosensory system, which is even more advanced than in other mammals, it is expected that manatees are familiar with pain. Moreover, we still do not know enough about their stress, fear, memory and pleasure systems, which all play a role in pain processing.
It would be great if we managed to achieve a better understanding of these amazing marine animals. But, until then, let us enjoy their existance peacefully, without interfering violently with their lifestyles and without exposing them to any potential pains.
For a more in-depth view on pain, as well as more information about manatees, I highly encourage you to read the papers and articles listed in References.
Special thanks to Isuru Priyaranga for creating the cover image. He is a fellow blogger and YouTuber, and I highly recommend visiting his blog and YouTube Channel.
References
- Neugebauer, V. (2007). Amygdala—Pain Processing and Pain Modulation. In: Zhuo M. (eds) Molecular Pain. Springer, New York, NY. doi:org/10.1007/978-0-387-75269-3_20
- Sarko, D.K., Johnson, J.I., Switzer, R.C., III, Welker, W.I. and Reep, R.L. (2007). Somatosensory Nuclei of the Manatee Brainstem and Thalamus. Anat Rec, 290:1138-1165. doi: org/10.1002/ar.20573
- Sneddon, L.U. (2017). Comparative Physiology of Nociception and Pain. Physiology, 33:63-73. doi:10.1152/physiol.00022.2017
- How did manatees inspire mermaid legends?
- A Manatee Was Found With ‘Trump’ Scraped Into Its Back
- Florida manatee with ‘Trump’ etched on back prompts investigation
- Manatees amid vegetation

The biological implications of meditation practices in the treatment of depression
Major depressive disorder (MDD) is a common mood disorder and a great cause of disability worldwide. Biological factors implicated in MDD range from neural imbalances to signaling dysregulations (which are partly grounded in genetic predispositions).
As shown in Figure 1, the socio-cognitive and biological deficiencies involved in MDD appear to influence each other in a circular, perpetuating manner. These deficiencies can be categorized into six non-exhaustive broad factors, i.e., mood, executive functioning, social skills, neuroplasticity, neural core networks, and neuroendocrine and neuroimmunological factors. The modulation of one factor is expected to exert an effect over the other factors, and subsequently to affect the overall depressive symptomology. Importantly, although these factors seem to play a causal role in the symptoms of MDD to various degrees, the precise causes of depression have not yet been entirely determined. There are, for instance, other psychological (e.g. cognitive biases) and biological factors (e.g. serotonin transporter genotype) that are known to be involved in depression, however these will not be covered in this article.

Particularly impaired in individuals with MDD is neuroplasticity, a crucial neural mechanism that entails structural and functional brain adaptations in response to altered environmental circumstances. This impairment is generally indicated by abnormally low levels of the brain-derived neurotrophic factor (BDNF), which is related to hippocampal and prefrontal atrophy in MDD. Moreover, impairments in stress regulation and immune system functioning have also been associated with the development of MDD symptoms. The following paragraphs describe in more detail the roles of BDNF, as well as those of cortisol, as a marker of stress, and of inflammatory cytokines in mental health, with a focus on depression.
BDNF is an important neurotrophin which promotes neuronal development, survival and plasticity in the central and peripheral nervous systems. It is most active in brain areas that play a role in learning, memory and higher cognition, such as the hippocampus and cortex. BDNF is also pivotal in the regulation of several physiological aspects, including stress response, mood, inflammation and metabolism. Decreases in BDNF levels have been linked to psychiatric and neurological disorders, such as depression, anxiety and Alzheimer’s disease.
Cortisol is a glucocorticoid secreted by the adrenal glands and, as part of the hypothalamic-adrenal-pituitary (HPA) axis, is a reliable marker for stress response. Cortisol is also part of the feedback mechanism in the immune system, where its role is to reduce certain aspects of the immune function, such as inflammation. Moreover, this hormone follows a robust circadian rhythm, which peaks 30 min after awakening, termed the Cortisol Awakening Response—CAR, and gradually declines throughout the day.
The circulating pro-inflammatory cytokines Interferon Gamma (IFN-γ), Interleukin-1β (IL-1β), Interleukin-6 (IL-6), Interleukin-8 (IL-8), Interleukin-12 (IL-12) and Tumor Necrosis Factor (TNF-α), as well as the anti-inflammatory cytokine Interleukin-10 (IL-10) have been extensively investigated over the past 20 years for their roles in depression, anxiety and various other chronic medical illnesses. Typically, decreases in inflammatory pathway activation during periods without active infection are associated with better physical and mental well-being. That being said, a general decrease in pro-inflammatory (and increase in anti-inflammatory) immune mediators is not necessarily indicative of health and wellness, since acute inflammatory responses are known to be adaptive; instead, a healthy homeostatic balance between pro- and anti-inflammatory signaling is most beneficial. Moreover, chronic inflammatory states can be triggered through psychosocial stress.
The deficits within these factors result in profound impairments in daily functioning, reduced quality of life, an increased risk of suicide, and a substantial lack of productivity. It is clear that there is a dire need to come up with alternative treatments for depression, next to the conventional first-line psycho- and pharmaco-therapies. One such alternative therapeutic strategy is meditation.
How meditation can alleviate the symptoms of depression ~ a biological standpoint
Mindfulness meditation is already being used in certain mental health facilities under different forms of psychotherapeutic intervensions, such as mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT). These usually consist of sessions guided by a professional in addition to at-home practice, over a duration of several weeks. While MBSR is tailored to the management of stressful situations, MBCT involves strategies for dealing with maladaptive thought patterns, which makes it more suitable for the prevention of depressive relapse. Upon repeated training, mindfulness meditation can lead to relatively global cognition-enhancing effects, as shown in Figure 2.
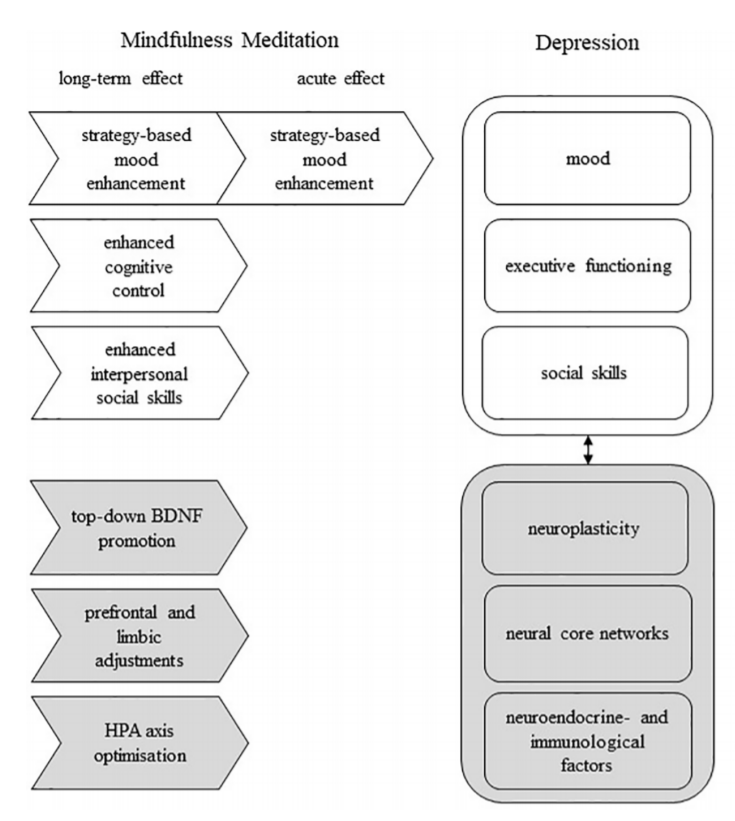
Adapted from Heuschkel and Kuypers (2020)
Meditative practices based on stress-reduction mechanisms and psychophysiological self-regulation are associated with anti-inflammatory benefits, through their modulation of inflammatory and HPA axis activities. In a study by Cahn et al. (2017), thirty-eight individuals participated in a 3-month yoga and meditation retreat, and were assessed before and after the intervention for psychometric measures, BDNF levels, circadian salivary cortisol levels, and pro- and anti-inflammatory cytokines. Participation in this yoga and meditation retreat was associated with better coping with stress, also known as stress resilience, as well as decreased self-reported depression, increased mindfulness, and generally enhanced well-being. The plasma levels of BDNF were increased by three fold post-retreat compared to pre-retreat, and this increase was inversely correlated with participants’ self-reported anxiety levels on a questionnaire (the Brief Symptom Inventory-18, BSI-18). In addition, the CAR levels were also significantly higher in these participants after the retreat, indicating improvements in the dynamic rhythmicity of the HPA axis activity, which is a marker of better stress resilience.
The researchers also found an unusual pattern of increases in both anti-inflammatory IL-10 as well as pro-inflammatory TNF-α, IFN-γ, IL-1β, IL-6, IL-8, with simultaneous decreases in the pro-inflammatory IL-12. While overall there are inconsistencies across studies on the influence of meditative practices on the immune system, it is also important to bear in mind that these studies tend to differ with respect to the type of intervention (e.g., Kundalini yoga vs. MBSR vs. Tai Chi), population (e.g., clinical vs. non-clinical), setting, design and other methodological factors; these differences lead to complexities involved in interpreting cytokine and other biomarker samples.
Having said that, pro- and anti-inflammatory response modulations may be adaptive depending on the context, for instance in chronically inflamed body states versus non-inflamed healthy normals. It is likely that in relatively healthy adults, intense yogic and meditative practices recruit an integrate brain-body response, resulting in enhanced pro- and anti-inflammatory signaling processes, which on the one hand support an upregulated vigorous immunological surveillance system, while on the other hand concomitantly promote high expression of the anti-inflammatory ‘‘break’’ such as IL-10.
Overall, the biological findings in the above-mentioned study correlate with enhanced stress resilience and well-being. At the end of an intensive three-month yoga-meditation retreat, the increased BDNF signaling and increased CAR were likely related to improved neurogenesis and/or neuroplasticity, and to enhanced alertness and readiness for mind-body engagement, respectively, while the higher levels of anti- and pro-inflammatory cytokines suggested better immunological readiness. Further research should attempt to investigate the role of other contextual factors (e.g., social dynamics, diet, natural environment, relative impact of a revered spiritual teacher etc.) impacting the expression and regulation of these biological processes.
To conclude, it is evident that meditation exerts beneficial effects on the brain. Particularly important to mental disorders, when meditation is used as a therapeutic intervention, it contributes to improving mental states and cognitive abilities by influencing several key biological factors crucial for normal brain functioning.
References
- Cahn, B.R., Goodman, M.S., Peterson, C.T., Maturi, R., Mills, P.J. (2017). Yoga, Meditation and Mind-Body Health: Increased BDNF, Cortisol Awakening Response, and Altered Inflammatory Marker Expression after a 3-Month Yoga and Meditation Retreat. Front Hum Neurosci, 11:315. doi: 10.3389/fnhum.2017.00315
- Dutta, A., McKie, S., Downey, D. et al. (2019). Regional default mode network connectivity in major depressive disorder: modulation by acute intravenous citalopram. Transl Psychiatry 9, 116. doi: org/10.1038/s41398-019-0447-0
- Heuschkel, K., & Kuypers, K.P.C. (2020). Depression, Mindfulness, and Psilocybin: Possible Complementary Effects of Mindfulness Meditation and Psilocybin in the Treatment of Depression. A Review. Front. Psychiatry, 11:224. doi: 10.3389/fpsyt.2020.00224
- Zeidan, F., Johnson, S., Diamond, B., David, Z., & Goolkasian, P. (2010). Mindfulness meditation improves cognition: Evidence of brief mental training. Consciousness and Cognition, 19, 597-605. doi: org/10.1016/j.concog.2010.03.014

The biology of meditation. How meditating can change your brain
Many of us are already familiar with what it means to meditate, in a broad sense, and we have often heard that meditation can improve our lives. Several books and articles have been written on the positive effects exerted by meditation on our bodies and minds. But what is the nature of meditation and how can it help us improve our mental states? More specifically, what happens at the level of neural networks, brain cells and molecules that results in all these beneficial actions upon meditating?
This being human is a guest house. Every morning a new arrival. A joy, a depression, a meanness, some momentary awareness comes as an unexpected visitor. Welcome and entertain them all! […] The dark thought, the shame, the malice. Meet them at the door laughing and invite them in. Be grateful for whatever comes. Because each has been sent as a guide from beyond.
The Guest House by Rumi. Translation by Coleman Barks

An introduction to meditation ~ its styles and purposes
Meditation encompasses various emotional and attentional regulatory practices, which aim at improving an individual’s cognitive abilities. Many recent behavioral, electroencephalographic and neuroimaging studies have investigated the neuronal events related to meditation, in order to achieve an increased understanding of cognitive and affective neuroplasticity, attention and self-awareness, as well as for their possible clinical implications.
The video below shows the kind of brain changes meditation leads to, in a monk who is a long-term practitioner.
According to Raffone and Sirivasan (2010), a central feature of meditation is the regulation of attention, and as such, meditation practices can be classified into two main styles—focused attention (FA) and open monitoring (OM)—depending on how attentional processes are directed. While the FA (‘concentrative’) style is based on focusing attention on a given object in a sustained manner, the second style, OM (‘mindfulness-based’) meditation, involves the non-reactive monitoring of the content of ongoing experience. More specifically, mindfulness refers to being constantly aware of the way we perceive and monitor all mental processes, including perceptions, sensations, cognitions and affects.
FA meditation techniques imply, apart from sustaining the attention on an intended object, monitoring attentional focus, detecting distraction, disengaging attention from the source of distraction, and (re)directing attention (back) on the object. This kind of attentional stability and vividness is achieved through concentrated calmness or serene attention, denoted by the word Samatha (which literarily means quiescence) in the Buddhist contemplative tradition. Another technique which can be broadly included in the FA meditation is transcendental meditation, which centers on the repetition of a mantra.
Unlike FA meditation, OM meditation does not involve an explicit attentional focus, and therefore does not seem to be associated with brain areas that control sustained or focused attention. Instead, OM meditation engages brain regions implicated in vigilance, monitoring and detachment of attention from sources of distraction from the ongoing stream of experience. Therefore, OM meditation is based on detecting arising sensations and thoughts within an unrestricted ‘background’ of awareness, without a ‘grasping’ of these events in an explicitly selected focus. In the transition from a FA to an OM meditative state, the object as the primary focus is gradually replaced by an ‘effortless’ sustaining of an open background of awareness, without an explicit attentional selection. In the Buddhist tradition, the practice of Vipassana (insight) OM meditation requires, first of all, attentional stability and vividness (acuity), as developed in FA meditation, in order to achieve a deep and reliable introspection.
The ancient yogic practice of Yoga Nidra, which is less-known, and yet is becoming increasingly popular, can also fall into the category of OM meditation. It is said to reduce stress and improve sleep, and that it has the potential to engender a profound sense of joy and well-being.
Another type of OM meditation worth mentioning here is the loving-kindness meditation or non-referential compassion (also known as Mettā in the Pali language), which involves compassion-based mental training aimed at promoting empathy. Practicing this kind of meditation is believed to increase the capacity for forgiveness, connection to others and self-acceptance, and to boost well-being and reduce stress. For more detailed descriptions as well as a deeper and broader understanding of the neurological implications of these different meditation practices, I strongly encourage you to check out the reviews listed in the Reference section, especially Brandmeyer et al. (2019) and Raffone & Srinivasan (2010).
Of all these different kinds, mindfulness meditation, which originally stems from Buddhist meditation traditions, has received the most attention in neuroscience research over the last twenty years.
Research over the past two decades broadly supports the claim that mindfulness meditation — practiced widely for the reduction of stress and promotion of health — exerts beneficial effects on physical and mental health, and cognitive performance.
Tang et al. (2015)
Sustained engagement with mindfulness meditative practices has been shown to have neurophysiological and psychological benefits. In healthy individuals, several months of mindfulness meditation practice correlates with improvements in self-regulation and subjective well-being. Even much shorter mindfulness meditation training, of a few days, has a positive impact on mood and executive functioning, while at the same time reducing fatigue and anxiety.
Brain structural changes following mindfulness meditation
Several recent studies have investigated the structural changes in the brain related to mindfulness meditation, and have reported alterations in cortical thickness, hippocampal volume, and grey-matter volume and/or density. However, before we dive into how meditation can change our brains, it should be mentioned that there are a few issues with the current state of meditation research. First of all, most of these studies have made cross-sectional comparisons between experienced meditators and controls. But only a few recent studies have investigated longitudinal changes in novice practitioners. These logitudinal studies are very important because they follow subjects over a long-term period of practice, and are thus able to determine whether changes induced by meditation training persist in the absence of continued practice. Therefore, more such studies would be required for a complete picture of the effects of meditation on mental health.
In addition, the studies on mindfulness meditation so far have generally included small sample sizes, of between 10 and 34 subjects per group, which leads to limitations in interpreting the results, as well as increases the chances of false-positives. Another prossible issue is that these studies use different research designs, measurements and type of mindfulness meditation. Hence, it comes as no surprise that the reported effects of meditation are diverse and cover multiple regions in the brain, including the cerebral cortex, subcortical grey and white matter, brain stem and cerebellum. That being said, these findings can also reflect the fact that the effects of meditation involve large-scale and interactive brain networks.
According to various fMRI studies, minfulness meditation exerts its effects primarily (though not exclusively) on a network of brain regions – the Default Mode Network (DMN). This network comprises structures in the medial prefrontal cortex (PFC), posterior cingulate cortex (PCC), anterior precuneus and inferior parietal lobule, which have been previously shown to have high activity during rest, mind wandering and conditions of stimulus-independent thought. These regions have been suggested to support different mechanisms by which an individual can ‘project’ themselves into another perspective.
When comparing meditators with naïve subjects, DMN regions, such as the medial PFC and PCC, have shown much less activity in meditators, across different types of meditation. This has been interpreted as indicating diminished self-referential processing. Experienced meditators also seem to exert stronger coupling between the PCC, dorsal anterior cingulate cortex (ACC) and dorsolateral PFC, both at baseline and during meditation, which indicates stronger cognitive control over the function of the DMN.
Brewer et al. (2011) investigated brain activity in experienced meditators versus meditation-naïve controls as they performed several different mindfulness meditations (Concentration, Loving-Kindness, Choiceless Awareness). They found that the main nodes of the DNM (medial PFC and PCC) were relatively deactivated in experienced meditators across all meditation types (Figure 2). Moreover, functional connectivity analysis revealed increased coupling in experienced meditators between the PCC, dorsal ACC, and dorsolateral prefrontal cortices, both at baseline and during meditation, as seen in Figure 3. This increased connectivity with medial PFC regions supports greater access of the default circuitry to information about internal states, because this region is also highly interconnected with limbic regions (such as insula and amygdala).


Meditators also reported significantly less mind-wandering, which has been previously associated with activity in the DMN. Therefore, these results demonstrated that alterations in the DMN are related to reduction in mind-wandering. They also suggested that meditation practice may transform the resting-state experience into one that resembles a meditative state – a more present-centered default mode.
The findings from this study have several clinical implications, given that a number of pathological conditions have been associated with dysfunction within areas of the DMN, including depression. The self-referrential function of the DMN has pointed to the possibility that excessive rumination (negative inner preoccupation about the personal past, present and future) in depression involves excessive DMN activity as well as an inability to switch out of it, in response to external demands. Mindfulness meditation may prove useful in reducing distractive and ruminative thoughts and behaviors, and this ability may provide a unique mechanism by which mindfulness meditation reduces distress and improves mood.
In addition, meditation has also been shown to promote neuroplasticity, an important neuronal process that entails structural and functional brain adaptations in response to changes in environmental conditions. A key neurotrophin that promotes neuroplasticity is the brain-derived neurotrophic factor (BDNF), which is usually found in abnormally low levels in various psychiatric and neurological disorders. Meditation has been shown to increase the levels of BDNF, thus promoting neuronal development, survival and plasticity, which in turn contribute to restoring the normal functioning of brain networks.
In sum, there is emerging evidence that mindfulness meditation might trigger neuroplastic changes in brain regions involved in the regulation of emotion and cognition. Although, as mentioned earlier, these studies often suffer from low methodological quality and present with speculative post-hoc interpretations, this is quite common in a new field of research. Thus, further research needs to use longitudinal, randomized and actively controlled research designs and larger sample sizes, as well as to concentrate on the biological factors implicated in mental health, in order to advance the understanding of how mindfulness meditation interacts with the brain. If supported by rigorous research, the practice of mindfulness meditation might be a promising therapeutic approach for clinical disorders, such as depression, and might facilitate the cultivation of a healthy mind and improved well-being.
For the readers interested in the effects of meditation on depression, please visit my article The biological implications of meditation practices in the treatment of depression.
References
- Brandmeyer, T., Delorme, A., Wahbeh, H. (2019). Chapter 1 – The neuroscience of meditation: classification, phenomenology, correlates, and mechanisms, Editor(s): Narayanan Srinivasan, Progress in Brain Research, Elsevier, 244: 1-29. doi: org/10.1016/bs.pbr.2018.10.020
- Brewer, J.A., Worhunsky, P.D., Gray, J.R., Tang, Y.Y., Weber, J., Kober, H. (2011). Meditation experience is associated with differences in default mode network activity and connectivity. Proc Natl Acad Sci U S A, 108(50):20254-9. doi: 10.1073/pnas.1112029108
- Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clin Psychol Sci Pract 10:144–156
- Heuschkel, K., & Kuypers, K.P.C. (2020). Depression, Mindfulness, and Psilocybin: Possible Complementary Effects of Mindfulness Meditation and Psilocybin in the Treatment of Depression. A Review. Front. Psychiatry, 11:224. doi: 10.3389/fpsyt.2020.00224
- Raffone, A., & Srinivasan, N. (2010). The exploration of meditation in the neuroscience of attention and consciousness. Cognitive Processing, 11:1-7. doi: 10.1007/s10339-009-0354-z.
- Tang, Y.Y., Hölzel, B.K., Posner, M.I. (2015). The neuroscience of mindfulness meditation. Nat Rev Neurosci, 16(4):213-25. doi: 10.1038/nrn3916
- Zeidan, F., Johnson, S., Diamond, B., David, Z., & Goolkasian, P. (2010). Mindfulness meditation improves cognition: Evidence of brief mental training. Consciousness and Cognition, 19, 597-605. doi: org/10.1016/j.concog.2010.03.014.

Forced to suffer for science: From animal cruelty and experimental inefficiency to a change of perspective.
We, as scientists, have become desensitised to the pain, the distress and the physical and emotional damage that we inflict on laboratory animals. So much so, that we constantly find justifications for our cruel experiments in the goal of finding cures for the illnesses of our conspecifics, and in the rules and regulations that authorise these heartless procedures.
Despite ongoing widespread use of animal models in research, recently there has been extensive criticism on the state of drug development in psychiatry, calling for a switch from rodent behavioral pharmacology to mechanistic studies in cellular systems. In a recent paper, Heilig and colleagues argue that:
Overall, neuroscience has simply had very little impact on clinical alcoholism treatment. The situation is representative of a broader translational crisis in psychiatric neuroscience. Because translational failures in this area have been the rule rather than the exception, pharmaceutical industry has largely retracted from efforts to develop novel psychiatric medication. As a result, the utility of animal models in research on psychiatric disorders, including addiction, is also being questioned.
Heilig et al. (2019)
Caricature Cruelty
Several experimental paradigms employed by labs all over the world, for elucidating the mechanisms of mental disorders and for the development of new psychiatric drugs, consist of procedures that innevitably cause suffering to the experimental animals. From learned helplessness paradigms (forced swim and tail suspension), intended to model the symptoms of depression in humans, to neuropathic pain models, which involve nerve operations to induce chronic pain in rats or mice, as well as fear conditioning experiments, consisting of series of electric shocks on consecutive days, large numbers of laboratory animals across the globe are subjected to procedures at the end of which they are euthanized for histological analyses.
The two videos below illustrate two paradigms for learned helplessness in rodents – forced swim and tail suspension, respectively. Even for those unfamiliar with these methods, it is not hard to notice the amount of distress and fear the animals are forced to go through.


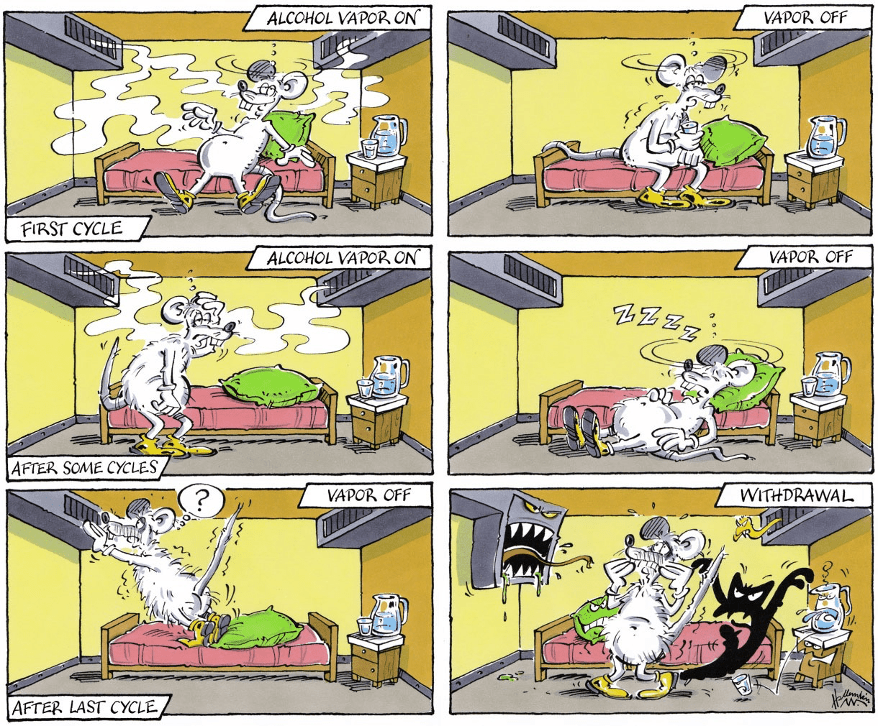
Another example, otherwise claimed to be minimally invasive and highly relevant for medication testing (Meinhardt and Sommer, 2015), is the post-dependent animal model, a model for medication development in alcoholism. It involves inducing dependence through repeated intermittent cycles of alcohol vapour exposure. In other words, rodents (usually, rats) are exposed every day, for several weeks or months, to cycles of intoxication with alcohol vapours, alternating with withdrawal, which ultimately result in compulsive alcohol intake, excessive alcohol seeking, hypersensitivity to stress as well as the development of an alcohol withdrawal syndrome, which better resemble human alcoholism.
Rats usually undergo 5 cycles of 14 (sometimes, 16) hours of forced exposure to alcohol vapours, separated by 10-hour periods of withdrawal and an additional 58 hours at the end of each weekly cycle. These cycles take place over many weeks. As a result of severe alcohol intoxication, some rats die during the experiment. At the end of the last alcohol exposure, the rats that have survived are decapitated.
The sardonically humorous caricatures below, selected from (Meinhardt and Sommer, 2015), not only illustrate the procedure, but are at the same time indicative of a certain emotional detachement these scientists have developed from the rats they used in their experiments.

“Unavoidable” Suffering
Granted, there have been attempts at reducing the suffering of these poor animals. The three Rs – Replacement, Reduction and Refinement – reflect the scope to encourage alternatives to animal testing, as well as improving animal welfare in experiments where the use of animals is unavoidable. The 3Rs have been incorporated into the legislation governing animal use in many countries, in order to ensure that the use of animals in testing is as ethical as possible.
And yet, with paradigms such as forced swimming test, also known as the behavioural despair test, or the tail suspension test ( where the rodent is hanging from its tail upside down and is unable to touch the walls of the compartment), it is clear that there is a big discrepancy between what could be done and what is actually being done. We could move away from these cruel practices, which have been demonstrated to be misleading and offer little understanding on the mechanisms behind psychiatric conditions, and, instead, resort to alternative strategies, which have the potential to set research on a path of true breakthroughs in psychiatry (as it is being presented in a later section). However, most papers focused on schizophrenia, anxiety, depression, Alzheimer’s disease, addiction etc. rely on experiments which would make the skin of the more sensitive of us crawl, and those with a tougher skin reconsider their academic career (such as switching to cognitive neuroscience and human-based studies only, in my case).
It is also important to remember that, not only the procedures themselves cause pain and suffering to the experimental animals, but often times the side-effects of the medications being tested on them and the behavioral tests they are being used in result in long-term health consequences – for instance, postdependent alcoholic rats end up developing peripheral secondary osteoporosis.
When suffering exceeds a certain limit, the animals are usually euthanized. What a great life these creatures must have, given that one of the best solutions to end their pain is premature death…
Rats empathise with other helpless rats
Although we all know that “animals have feelings too”, we are still far from understanding to what extent animals actually feel. In humans, for instance, pain and consciousness are tightly linked. We do not yet know which animals have consciousness and what (if anything) that consciousness might be like.
That being said, a study from 2011 demonstrated that rats exhibit emotional responses and empathy. In their experiment, Bartal and colleagues showed that when a free rat occasionally heard distress calls from another rat trapped in a cage, it learned to open the cage and released the other animal even in the absence of a payoff reunion with it. The free rat would even save a chocolate chip for the captive.
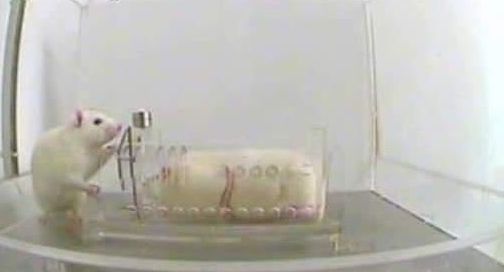

The presence of a rat trapped in a restrainer elicits focused activity from his cagemate, leading eventually to door-opening and consequent liberation of the trapped rat. (Science/AAAS).
This experiment clearly shows that rats, and possibly other animals as well, are capable of complex emotional experiences, previously only attributed to humans (more studies should be done to investigate this fascinating and important topic). Alas, in the absence of a deep understanding of the animal psyche, and moreover, with clear indications that animals possess the capacity to feel almost to the same extent as us humans do, we still continue to abuse them in our cruel experiments.
The issues with animal models
Valid disease models do not exist for psychiatric disorders.
Hyman (2012)
On the rodent models based on learned helplessness, Hyman went on to argue that:
Forced-swim and tail suspension tests do not even model the therapeutic action of antidepressants, because in those rodent screens a single dose of antidepressant is active, whereas in dependent patients, antidepressant drugs require weeks of administration to exert a therapeutic effect.
Hyman (2012)
In fact, given that most psychiatric diseases are heterogenous and polygenic, often times animal behavioral models have turned out to be misleading. Shockingly, only 8% of the CNS drug candidates developed between 1993 and 2004, which reached initial human testing, were approved to be used as medication. The main drawbacks of these drugs were the toxicity discovered in late-stage clinical trials, along with the inability to demonstrate efficacy. Not to mention the serious side effects these drugs produce in humans, such as weight gain and metabolic derrangements.
Animal models, albeit useful for some translational investigations and for basic studies in neuroscience, present various limitations:
- Lack of molecular and neural circuit-based characteristics, which are required for molecular studies of psychiatric diseases.
- The construction of transgenic mice is too slow and expensive.
- Regarding non-human primates, the challenges involve cost, less well-developed technologies as well as ethical barriers.
- When it comes to invertebrate models or zebrafish (extensively used in translational research), evolutionary distance poses huge obstacles in translational psychiatry, although they could be useful in the initial molecular investigations of the functions of risk alleles emerging from genetic studies.
Given the above-mentioned drawbacks of relying on animal models to develop psychiatric treatments, major pharmaceutical companies have already decided to move away from these old-fashioned approaches. Now, the question remains, what is there to do in the future?
Adopting new strategies in psychiatric research
Science needs to move forward and find better methods to study the highly complex mechanisms underlying psychiatric diseases, in order to allow for truly efficient drugs and therapies to be developed. As mentioned earlier, animal-based studies have more often than not failed to identify pharmaceutical compounds with positive outcomes in humans.
Over the last half-century, despite the identification of several antipsychotic and antidepressant drugs, alongside the discovery of various neurotransmitters, receptors and transporters involved in mental illnesses, objective diagnostic scans are scarce, and, surprisingly, only a handful of validated molecular targets have been established.
Luckily for us, there are several alternative solutions, which are already being seriously considered by various laboratories and drug companies, as listed below:
- DNA sequencing, which is nowadays much cheaper than it used to be (by 1 million-fold), makes it possible to analyse large number of subjects, in the attempt to identify genes involved in the heterogenous, polygenic psychiatric disorders.
- Large scale studies of gene function, epigenetics, transcriptomics and proteomics would contribute to the understanding of pathogenesis.
- Optogenetics, a technology with increasing popularity in neurobiology, allows researchers to activate or inhibit single cell types, thus detecting which circuits are specific to certain disorders.
- Human neurones derived directly from skin fibroblasts and blood cells in vitro, or generated from human embryonic stem cells (hESCs) or induced pluripotent stem cells (iPSCs) in vitro.
- These above-mentioned tools can be combined with electrophysiological and neuroimaging data from humans, which can indirectly reveal abnormal functioning of widely distributed circuits.
What psychiatric research needs is to be able to accurately model molecular mechanisms of disease, instead of relying on behavioral results. Since I already mentioned large-scale genetic as well as epigenetic strategies, it is fair to admit that such studies require suitable living systems in which experiments can be conducted (given that the living human brain is not accessible, and that postmortem studies have limitations when it comes to functional analyses). Although, in some circumstances, animal behavioral experiments can help in elucidating treatment options, conclusions ought not to be based on modelling disease symptoms, as these can be misleading and often fail to translate into human psychopathology. Moreover, symptoms change over time and depending on the context, and are based on subjective rating scales, making the comparison between human and animal conditions difficult.
The solution is plain and simple – scientists and pharmaceutical companies must, first of all, unanimously and once and for all come to terms with the fact that the efforts based on cruel animal studies have been of too little avail to justify their continuation. Instead, a new strategy must be incorporated by the scientific community in psychiatric research, which should carry on from cell-based models and established molecular mechanisms to early human trials, skipping the intermediate step of animal behavioral models.
To end on a cheerful note, here is a heartwarming video which proves there is hope that the future could look bright for laboratory animals if people are willing to start making a change:

Special thanks to my mom for insightful comments and for her constant support, and to Gasser Elmissiery for inspiring discussions and for his contribution to creating the featured image.
References
- Bartal, I. B.-A., Decety, J., & Mason, P. (2011). Empathy and Pro-Social Behavior in Rats. Science, 334(6061), 1427 LP – 1430. doi:org/10.1126/science.1210789
- Haaranen M, Scuppa G, Tambalo S, Järvi V, Bertozzi SM, Armirotti A, Sommer WH, Bifone A, Hyytiä P. (2020). Anterior insula stimulation suppresses appetitive behavior while inducing forebrain activation in alcohol-preferring rats. Transl Psychiatry. 10(1):150. doi: 10.1038/s41398-020-0833-7
- Hansson AC, Koopmann A, Uhrig S, Bühler S, Domi E, Kiessling E, Ciccocioppo R, Froemke RC, Grinevich V, Kiefer F, Sommer WH, Vollstädt-Klein S, Spanagel R. (2018). Oxytocin Reduces Alcohol Cue-Reactivity in Alcohol-Dependent Rats and Humans. Neuropsychopharmacology. 43(6):1235-1246. doi: 10.1038/npp.2017.257
- Heilig M, Augier E, Pfarr S, Sommer WH. (2019). Developing neuroscience-based treatments for alcohol addiction: A matter of choice? Transl Psychiatry. 9(1):255. doi: 10.1038/s41398-019-0591-6
- Hyman SE. (2012). Revolution stalled. Sci Transl Med. 4:155cm11
- Knobloch HS, Charlet A, Hoffmann LC, Eliava M, Khrulev S, Cetin AH, Osten P, Schwarz MK, Seeburg PH, Stoop R, Grinevich V. (2012). Evoked axonal oxytocin release in the central amygdala attenuates fear response. Neuron. 73(3):553-66. doi: 10.1016/j.neuron.2011.11.030
- Meinhardt MW, Sommer WH. Postdependent state in rats as a model for medication development in alcoholism (2015). Addict Biol. 20(1):1-21. doi: 10.1111/adb.12187
- Wahis, J., Kerspern, D., Althammer, F., Baudon, A., Goyon, S., Hagiwara, D., … Charlet, A. (2020). Oxytocin Acts on Astrocytes in the Central Amygdala to Promote a Positive Emotional State. BioRxiv, 2020.02.25.963884. doi:org/10.1101/2020.02.25.963884

Volunteering in Sri Lanka
In this article, I will tell you guys about my clinical experience in an extotic and remarkable country.
In November 2018, I completed a four-week Mental Health Foundation Placement in Sri Lanka, as a volunteer for the organisation SLV.Global.
When I decided to join this placement, I was extremely interested in the culture of this small country at the bottom of India, which I had often heard being referred to as “the Pearl of the Indian Ocean”. At the same time, as a final-year undergraduate Neuroscience student, I was looking for a more clinical, psychology-based experience, and was fascinated by the idea of volunteering in mental health, in a country that seemed to be in great need of such work.
A bit about Sri Lanka
Sri Lanka has an extraordinary cultural, ethnic and natural diversity, as well as a long and distinguished history.

Map of Sri Lanka
Religion is very important. This country is the home of one of the world’s oldest and purest forms of Buddhist traditions, approximately 70% of the population being Buddhist. 12.6% are Hindus, especially in the North and East of the country, 9.7% Muslims, and 7.4% Christians. In 2008, Sri Lanka was the third most religious country in the world according to a Gallup poll.
Ethnically, there are two main groups of population, with different languages, the Singhalese (most of them of Buddhist religion and speak Sinhala) and Tamils (mainly Hindus and speaking Tamil). Apart from these, there are also the Moor of Arabic descent, Burghers (descendants of European colonists), Malays and ethnic Chinese migrants who came to the island in the 18th and 19th centuries.
Another name of Sri Lanka is Ceylon. Many people around the world are familiar with this name, due to the Ceylon tea (green and black tea), from the vast upland plantations in Sri Lanka. But the Ceylon tea is just one of the many natural riches that make this tiny island a tropical paradise.
For tourists, Sri Lanka has it all – from very well-conserved ancient vestiges to beautiful beaches, amazing landscapes, impressive temples and incredible flora and fauna, many of which are endemic.

One of the entrances to the Temple of the Sacred Tooth Relic in Kandy. The interior of the temple is truly spectacular and quite intricate in its structures and decors.

Sigiriya (Lion Rock), one of the medieval Sri Lanka’s most remarkable royal palaces and an unforgettable landmark.

Dancers performing the famous Kandyan dance.
But many of those who visit this small Indian Ocean country only for touristic purposes sadly overlook the struggles of its inhabitants, reflected, among others, by the issues in the educational and health care systems, widespread poverty, socio-political confusion rising from the centuries-long colonial history (until Sri Lanka’s independence in 1948), and the ethnic problems.
Mental health problems in Sri Lanka
Sri Lanka deals with an increasing prevalence of mental illness and a high suicide rate. Suicide is the second biggest cause of morbidity and unnatural death. In 2016, Sri Lanka ranked number 31st in the world for the suicide rate. This situation is largely determined by poverty and the traumas caused by a 26-year civil war which only came to an end in 2009. In addition to these, in 2004 the country was devastated by a tsunami, which led to about 35,000 deaths and 516,000 displacements, and which has contributed to the high rate of PTSD, anxiety and depression. Schizophrenia affects around 210,000 people, based on a report by the World Health Organisation, in 1993.
By contrast, Sri Lanka has great deficit in mental health resources, funding and clinical staff. Only 1% of the government funds is directed to the mental health sector. Currently in Sri Lanka, there are only 89 psychiatrists serving a population of 21 million, and the number of other mental health professionals (psychiatric nurses, psychologists, occupational therapists etc.) is also extremely low.
One of the main causes for the lack of personnel is the stigma attached to mental illness which is perceived as shameful.
People with depression and attempted suicide are subject to discrimination, for instance when seeking a job. The relatives of the mentally ill themselves consider them a burden and abandon them. There are cases of patients after being discharged from the hospital and upon returning home, they were rejected by their own families and left homeless, which determined them to return to the hospital, as that became their only home. In fact, a friendly family environment and a society without the above-mentioned prejudices would allow a successful recovery of the patient.
Stigma affects not only the ill, but also the mental health professionals. The latter are being looked down upon, and so, many of them choose to leave the country and work abroad. Other significant consequences of stigmatisation are the lack of proper training of the mental health staff, as well as the very little advancement of the psychiatric treatment, which in Sri Lanka is mainly reduced to medication and electroconvulsive therapy.
There is need for a change in mentality, so that mental illness stops being considered shameful, and instead it is seen as any other disease, like cardiac or liver diseases. At the same time, it would be necessary that the government, too, take the problem of mental health more seriously, and allocate more resources to it.
It is remarkable the fact that some Sri Lankan psychiatrists have already taken steps in changing the mentality, by organising workshops about mental health in schools and for their patients’ families.
Our projects
The projects run by SLV.Global, in partnership with the mental health charity Samutthana Kings College London Centre for Trauma, Displacement and Mental Health, support the very few local mental health professionals in their attempt to fight the stigma around mental illness, promote alternative therapeutic approaches, and help former patients reintegrate in their community after being discharged from the hospital.
Volunteers stayed at local Sri Lankan families at three different locations – Colombo, Kotte and a rural area called Horana and Bandaragama (I lived in Horana and Bandaragama). This was very important to us, because it helped us better understand Sri Lankan customs and mentalities.
We ran seven sessions per week. The first week was, however, dedicated entirely to the volunteers’ orientation. We participated in workshops with mental health professionals about working with service users, effective session planning, and the mental health situation in Sri Lanka. One of the workshops took place in a Buddhist Thai Temple, where a Buddhist monk gave us tips on meditation, which we were then able to include in some of the therapy sessions we ran.
The projects took place in a number of different facilities (centres for special needs, vocational training centres, schools, temples, psychiatric hospitals etc.), with service users having a variety of different diagnoses. The sessions we organised focused on enhancing the social skills, communication skills, motor and sensory functioning, and cognitive skills (e.g. short-term and long-term memory, sustained attention, learning, imaginative play) of the service users. Activities included performing dancing routines, yoga for relaxation and mindfulness, musical activities, movement therapy sessions, games (e.g. puzzles, board games).
The main goal of the sessions was to improve the quality of life of the service users, by increasing their general well-being, and supporting them to develop skills that they could use to become more financially and socially independent.
During my volunteering in Sri Lanka, one of the things I truly valued was the fact that the people we volunteered for were referred to as service users (not “patients” or “mentally ill”). This was due to the attempt at changing the mentality around mental illness, by helping the service users feel less like patients and more like any other human being, who deserves respect, love and appreciation.
It was also interesting to see that the sessions we ran included meditation (relaxation yoga, laughing yoga) and breathing techniques, rather than being solely based on Western forms of therapy, which indicated attempts at an integrative approach to mental health.
The projects we worked on were often challenging, as the service users suffered from a variety of conditions, from communication and intellectual impairments to schizophrenia and depression, and we did not have access to any individual service user’s diagnosis or history, since we were not members of the clinical staff. Therefore, we had to figure out by ourselves what best worked for each of them.
Aside from activities aimed at promoting mental health, volunteers also took part in English for Development projects, which took place in schools, temples, community centres and vocational training centres. These sessions focused on improving the spoken English and communication of students, which would prove very useful for studying or having a job in their home country, as well as abroad.
Creativity was the key
All volunteers had access to the session planning sheets, materials and ideas used in the past by previous volunteers, but were encouraged to be creative and come up with their own ideas.
During this placement, I decided to use classical music, particularly Baroque pieces, in sessions aiming at improving memory and social interaction. For example, in one session my group of volunteers had the service users at that respective facility (who were suffering from communication impairments, intellectual disability and depression) listen to several classical compositions, and then associate these with drawings of faces representing various moods or feelings. Service users were also encouraged to tell us why, to them, a musical piece evoked a certain feeling. The scope of this activity was to expose the service users to classical music (known for its benefits on the mental processes) and help them form associations between auditory and visual stimuli.
Another innovative idea, which two of my teammates had, was to use Kendama toys as a means of improving fine motor skills, coordination and forward planning, as well as a stress relieving mechanism. We soon discovered that certain service users suffering from depression and autism-spectrum disorders had become more receptive, more talkative and less aggressive after a few sessions combining Kendamas and classical music.
Ayurvedic medicine and modern medicine

The Golden Temple of Dambulla.
Sri Lanka relies heavily on traditional medical practices based on Ayurveda (Ayurvedic medicine), astrology and religion (mainly Buddhism).
The Ayurvedic medicine involves, among others, the use of herbs, meditation, massages and special diets, in order to prevent and cure disease, increase wellbeing, and decrease stress. The Ayurvedic belief is that health problems are due to a disharmony between mind, body and spirit, and that restoring the balance will restore and maintain health. Establishing one’s diagnosis is based on the person’s medical history, emotions, relationships with other people, and a close examination of different parts of the body. The treatment is then established according to what the practitioner decides best suits the individual.
Alongside traditional medical practices, there are of course modern Western forms of psychiatry and care. One of the largest institutions dedicated to mental health is The National Institute of Mental Health (NIMH) located at Angoda, Kandy District, founded in 1927 and having a capacity of 1,500 beds.
The two approaches, Ayurvedic medicine and Western medicine, should not be seen as opposites. It is clear that both of them have limitations, which is why mental illnesses still persist, and some are even rising. We have to admit that Western doctors are reluctant about ayurvedic medicine. Among the critiques they have provided of ayurvedic medicine are the fact that it is not very scientific, it can have severe side effects, and can interfere with conventional treatment. However, modern approaches, too, have offered neither conclusive answers to questions about the causes or triggers of mental disorders, nor definitive solutions to curing them. In my opinion, instead of rejecting ayurvedic medicine or ridiculing it, we should try to know as much about it as possible, and then decide whether it is suitable or not.
I believe that a great challenge is integrating the Occidental and Oriental views. Sri Lanka is one of the countries with a long-lasting experience in ayurvedic practices, which makes it one of the few ideal places where reconciling the two medical approaches could be successful.
Final thoughts
I left Sri Lanka with the hope that one day I can go back to work in mental health there, and that I can convince more people to do the same. While volunteering there, it soon became clear to me that, in a land where where mental illness is still a taboo topic, volunteers contribute to the wellbeing of the service users simply by their presence. If more people with experience and knowledge in Psychology, Psychiatry and Neuroscience, and who have a genuine desire to help others, volunteer in Sri Lanka, the costs involved in psychiatric treatment there would decrease, alternative forms of treatment would start to spread, and more awareness will be raised about the importance of mental health.
To me, this experience was not only an opportunity to make myself useful, but above all, it was a learning and an eye-opening experience.
When volunteering in Sri Lanka, it is very important to understand the culture, the traditions and the customs there, and try to think outside of the box. An integrative approach, where modern Western forms of medicine and Eastern, more traditional, practices are combined, would benefit not only Sri Lankans, but the volunteers themselves and their own communities. As volunteers, we can bring back to our countries what we learn in Sri Lanka, and help improve our still-in-progress medical system.
I would like to thank Prof. Aravinda Ravibhanu Sumanarathna, Senior Research Development Scientist at Institute of Professional Studies & Skill Development Sri Lanka, CEO & Founder of Eco Astronomy Sri Lanka Research Unit, and Isuru Priyaranga Silva, BSc. Microbiology student and Eco Astronomy Researcher, as well as their lovely families, for making me feel like home when I was so far away from mine, for offering me valuable information about Sri Lanka, for showing me its beauties, and for revealing to me the well-known Sri Lankan hospitality.
I am also thankful to my homestay family, Uditha Dananjani and Sampath Dissanayake, and to all the Sri Lankan volunteers I had the great pleasure to work with, especially to Gayeshi Lakshika who helped me many times practise Sinhala.
I also thank Prof. Hugh Piggins, Head of School of Physiology, Pharmacology and Neuroscience, University of Bristol, for supporting and encouraging me to volunteer in Sri Lanka.
References
De Silva, D. (2002). Psychiatric service delivery in an Asian country: the experience of Sri Lanka, International Review of Psychiatry, 14:1, 66-70, DOI: 10.1080/09540260120114096
Hutter, C., Haputantri, M., Anver, G. (2016). Inside Sri Lanka’s National Mental Health Institute: A Photostory. Retrieved from: https://roar.media/english/life/reports/inside-sri-lankas-national-mental-health-institute-photostory/
Minas H., Mendis J., Hall T. (2017). Mental Health System Development in Sri Lanka. In: Minas H., Lewis M. (eds) Mental Health in Asia and the Pacific.International and Cultural Psychology. Springer, Boston, MA.
Uduman, N. (2018). Mental Health and Stigma in Sri Lanka. Retrieved from: https://groundviews.org/2018/02/19/mental-health-and-stigma-in-sri-lanka/

Oxytocin and Social Bonding
While most of us would be able to describe what being affectively close to someone feels like, we might find it harder to explain why and how such a connection forms.
Why do we love and what makes us love certain people? Why is love so different depending on the subject of our affection? Is it possible to measure love? What does the complete absence of love in an individual reveal about their health state? With so many questions having been formulated throughout centuries, no wonder love has become a universal conundrum. Traversing various disciplines, it not only represents the realm of the literary, but it has increasingly become one of the central focuses in philosophy, biology, social sciences and neuroscience.
As far as the neuroscientific approaches to love go, this concept is represented by affiliative bonds. Therefore, from now on we shall refer to love as such. For the sake of the reader’s personal interest, we shall further discuss affiliative interactions as they appear and manifest in humans. Affiliation describes the ability of an individual to form close interpersonal bonds with other individuals of the same species. Three prototypes of affiliation have been identified: parental (between children and their parents), pair (between romantic partners) and filial (between friends).
This article is intended to introduce the reader to the evolutionary significance and neurochemical mechanisms underlying social bonding/affiliation. As such, the above-mentioned types of affiliative behaviours will be only in part separately discussed. Instead, we shall focus on what these categories share in common, particularly, the hormone-neurotransmitter oxytocin and the concept of synchrony.
Synchrony refers to the process by which the members of a social group collaborate with each other, in order to achieve a social goal. This kind of collaboration involves concordance in time between members, at the level of behaviour and physiological processes (e.g. hormonal release, neural firing). Through these synchronous processes underlying social reciprocity, each member is introduced to the social milieu, becomes adapted to his/her environment and learns how to survive.
Intimate reciprocal relationships between two individuals in a social group help shape the individual’s moral, empathic and pro-social orientation, as well as social adaptation and self-regulation. The interaction between mother and infant is critical to the social maturation and well-being of the young. Human mothers, just like other mammals, exhibit specific postpartum behaviours, such as affectionate touch, high-pitched vocalisations, expressing positive affect, which lead to the notoriously strong mother-infant bond.
This type of specific attachment relationship coordinates the physiology of the infant with the behaviours of the mother. Moreover, this mother-infant synchrony enables the temporal alignment of the infant’s inner state with the responses of the social environment (via the mother). The absence of a proper interaction between mother and child, especially within the critical period (between 3 and 9 months after birth), has been shown to contribute to the development of autism spectrum disorders (for more information on autism, check out this previous article – Decoding autism).
Romantic attachment is another type of social bonding in humans, with significant implications to the normal psychological functioning of the individual. According to recent studies, both parental and romantic relationships share similar behavioural characteristics (gaze, touch, affects, vocalisations and coordination of these behaviours between the members of the pair) and rely on similar neuroendocrine mechanisms. These mechanisms mainly involve a nine amino-acid neuropeptide known as oxytocin.
Oxytocin acts as both a hormone and a neurotransmitter. It is associated with a variety of functions including the initiation of uterine contractions during parturition, homeostatic, appetitive and reward processes, and last but certainly not least, the formation of affiliative bonds. For the latter, oxytocin plays a very important role in social recognition, maternal behaviour and development of partner preferences.
Oxytocin is produced in the hypothalamus, by the magnocellular neurones clustered in two types of nuclei: the supraoptic and paraventricular. These neurones send projections to the posterior pituitary gland, thus engaging the oxytocin system with the hypothalamic-pituitary-adrenal axis, mediating the stress response, as well as parturition, lactation and milk ejection. Other projections from the paraventricular nucleus go to various forebrain limbic structures (e.g. amygdala, hippocampus), brainstem (e.g. ventral tegmental area) and spinal cord. There are also other areas, apart from the brain and spinal cord, which receive oxytocin signalling, such as the heart, gastrointestinal tract, uterus, placenta, testes etc. With such extensive projections, it comes as no surprise that oxytocin is involved in a wide variety of processes.
In romantic and parental attachment, oxytocin induces the motivation to initiate sexual behaviour, the formation of sexual preferences and the increased stimulant value of the infant for its mother, via its connectivity with the mesolimbic dopaminergic neurones. The neurotransmitter dopamine plays a major role in the reward-motivated behaviour. Therefore, the oxytocin-dopamine interaction is key to the motivation to bond between members of romantic or child-parent relationships.
If you were wondering why the parental attachment has so far been presented only from the perspective of the mother-child relationship, that is because in males a different hormone mediates parental behaviour. Vasopressin can be seen as the male equivalent of oxytocin, as it modulates affiliation, aggression, juvenile recognition, partner preference and parental behaviour in males. Having said that, there are studies which show that oxytocin also supports paternal behaviour and is linked to the father-typical affiliative behaviour.
Oxytocin is also very important in establishing close connection with our best friends (what is known as filial attachment). According to research in this area, children start showing selective attachment to a ‘best friend’ around the age of 3. This kind of interpersonal interaction represents the first attachment to non-kin members of society, therefore, a crucial step in the normal development of any human being.
Depending on the level of synchronous parenting children experienced during infancy, their interactions with best friends can vary in the degree of reciprocity, emotional involvement and concern for the friend’s needs. These behaviours are modulated by oxytocin. During the first 3 years of life, oxytocin secretion in humans depends on the parent’s postpartum behaviour (which is predicted by the parents’ own levels of oxytocin) and, in turn, determines the degree of empathy between close friends. Therefore, a reasonable assumption, which has been recently proven, is that children benefiting from high parental reciprocity during infancy develop better social adaptation, are more friendly and cooperative, and show greater empathy.
All in all, the social bonds we form with members of our social group, be they our family, romantic partners or friends, are dependent on certain hormones and behaviours occurring at critical stages of development. Close attachment bonds with our parents, during early infancy, are later translated into affiliations to non-kin members of the social groups, who we come across during childhood, evolving into intimate friendships during adolescence, which eventually shape the ability of the adult human to form and maintain romantic connections and provide nurture for the next generation.
What we have just discussed is of importance for different aspects. Focusing on oxytocin and synchrony provides better understanding of neurodevelopmental disorders such as autism. At the same time, this focus offers some answers to questions regarding the reasons and mechanisms underlying the many types of love us humans experience throughout our lives.
References
Feldman, R. (2012). Oxytocin and social affiliation in humans. Hormones and Behavior, 61(3), 380-391.
Hammock, E. A. ., & Young, L. J. (2006) Oxytocin, vasopressin and pair bonding: implications for autism. Philosophical Transactions of the Royal Society B: Biological Sciences, 361(1476), 2187–2198.

Fear and the amygdala
What is fear? Why are we sometimes afraid? Can fear be inhibited? What produces fear – the brain or the heart?
It is definitely the brain! More exactly, something in the brain – a tiny, almond-shaped structure, which sits anteriorly to the hippocampus, called the amygdala. This small part of our brain is to blame for the perception of fearful stimuli and the physiological responses (increased heart rate, electrodermal responses etc.) to fearful stimuli.
As part of the FEAR system, the amygdala connects to the medial hypothalamus and the dorsal periaqueductal grey matter (in the midbrain), which is important in pain modulation in the dorsal horn of the spinal cord, as well as to sensory and association cortices. The lateral nucleus of the amygdala receives inputs from different brain regions, thus allowing the formation of associations, required for aversive conditioning. Following the processing in the lateral nucleus, information about the stimulus is, then, projected to the central nucleus of the amygdala, where an appropriate response to the stimuli is initiated, provided that the stimuli are detected as threatening or potentially dangerous.
The amygdala is involved in emotional learning and memory, modulating implicit learning, explicit memory, attention, social responses, emotion inhibition and vigilance.
You can find the article on memory here, to brush up a bit.
- Implicit memory is a type of learning, which cannot be voluntarily reported or remembered. It includes the memories for skills and habits, for procedural knowledge, grammar and languages, priming, simple forms of associative learning and classical conditioning. The latter is particularly important for fear. It involved a conditioned stimulus (CS) and an unconditioned, painful/fearful stimulus (US), with US preceding CS and determining a fearful response to CS. This type of fear learning is adaptive and is known as sensitisation or acquisition.
There are two different pathways in the amygdala, important for fear conditioning. The “low road” pathway: sensory information projects to the thalamus, which directly communicates with the amygdala; this pathway is fast, modulating rapid responses of the amygdala to different types of fearful stimuli. The “high road” pathway is an indirect pathway: sensory information projects to the thalamus and from there, it is conveyed to the sensory cortex for a finer analysis; the sensory cortex, then, communicates the processed information to the amygdala. This pathway ensures that the sensory stimulus is the conditioned stimulus. So the responses of amygdala to threatening stimuli are both rapid and sure.
- Explicit memory refers to the memory of facts and events; in the case of fear is means the processing and retention for a long time, of emotional events and information. For this type of fear learning, the amygdala interacts with the hippocampus. There is a distinction between the formation of memory for aversive experience (fear conditioning), which is based on previous experience, and explicit learning (in the hippocampus), which involves learning and remembering aversive properties of different threatening stimuli. The memory in the hippocampus is enhanced by arousal produced in the amygdala. The activation of the amygdala can make different cortical areas, not just the hippocampus, more receptive to stimuli that are adaptively important, thus ensuring that unattended, but important stimuli gain access to consciousness.
- Social responses involve the ability to recognise a stimulus as good, bad, neutral or arousing. This ability, however, does not depend on the amygdala. There is one exception here, otherwise we wouldn’t be talking about it in the context of fear mediated by amygdala – fearful facial expressions. According to Darwin, social species, like humans, use facial expressions to detect internal emotional states of other members of the group. This function, mediated by the amygdala, is crucial in the emotional regulation of human social behaviour. Damage to amygdala has been demonstrated to result in impairment of the patient to identify fearful faces correctly and, therefore, react to them, accordingly. It should also be noted there is no need for the subject’s awareness of the fearful stimulus, for the amygdala to respond. In other words, when a fearful facial expression is presented subliminally, the amygdala will still show activation.
- Inhibition of fear – it is actually very difficult to escape your own fears, as fear proves to be resistant to voluntary control. However, there is a process called extinction, a method of classical conditioning, where a CS previously associated with an aversive US in presented alone for a number of times, until the CS no longer signals the fearful stimulus. If the US is presented again, after the passage of time, it will evoke fear responses, but in different brain areas. So, the learned fear has been retained in memory, but extinction learning eliminates the response to fear. This mechanism of extinction relies on the activity of NMDA glutamate (excitatory) receptors in the amygdala. When these receptors are blocked, extinction is inhibited (so you will react to fearful stimuli) and when they are active, extinction is augmented (you no longer respond to aversive stimuli).
- Vigilance – the amygdala is not necessary for the conscious experience of emotional states, but it plays a major role in increasing the vigilance of cortical response systems to emotional stimuli.
Memories about fearful events, just like other types of long-term memory, become permanent through a process of gene expression and novel protein synthesis, which is known as consolidation. Upon retrieval, the memories become susceptible to change and alteration, before they are reconsolidated, which involves additional protein synthesis.
The fact that humans (and probably other animals as well, I am sure, although not widely proven) have the ability to distinguish between emotional information and unemotional information is regarded as an evolutionary advantage. Emotional stimuli signal dangers and the ability to detect and appropriately react to them increases the chance of survival. However, exacerbated fear is detrimental to the individual who experiences it and is a sign of pathology. For instance, in atypical monopolar depression, which includes anxiety as one of the main symptoms, the amygdala is overactive and it determined lowering the threshold for emotional activation and abnormal reactions to stressful stimuli. A similar pattern can be seen as a result of partial chronic sleep deprivation or complete acute sleep deprivation.
References
Beatty, 2001. The Human Brain – Essentials of Behavioural Neuroscience, Sage Publications Ltd., pg. 293-296
Bernard et al., 2007. Cognition, Brain and Consciousness – Introduction to Cognitive Neuroscience. 1st edition. Elsevier Ltd., pg. 373-383
Gazzaniga et al., 2002. Cognitive Neuroscience – The Biology of Mind. 2nd edition. W.W Norton & Company, Inc., pg. 553-572
Image by Saya Lohovska. You can find her arts page here.

Consciousness – Who decides, 𝘺𝘰𝘶 or your brain?
If you were to answer the question “What differentiates humans from other organisms on Earth?”, you would probably list a number of things, including the ability of humans to make “free choices” dictated by their consciousness, rather than by something organic. Am I right?
What if someone told you that this is not actually the case? I mean, what if instead of making decisions out of your own will, your brain is “deciding” for you and only after the decision has been made the brain offers you the illusion of conscious act, making you believe that you were the one who made the choice in the first place. But how is it possible that such a dichotomy exists within ourselves, between us and our own brains? Aren’t we our brains? Apparently not!
Now that I (hopefully) managed to capture your attention, I’d like to bore you a bit with some brain structure names and functions, which are necessary in order to begin to understand what’s going to come next.
The frontal lobe contains a few areas, which are involved in planning our movements, decision-making, emotions (usually associated with the decisions we are about to make), repeating previously memorised motor sequences etc. These are the areas involved in voluntary motor control, more specifically, these are the areas that make the difference between reflexes/automatisms and movements or actions we want to pursue. Moreover, all these motor areas are interconnected and also linked to areas that are part of the sensory pathways, such as the parietal , visual, somatosensory and temporal regions (which store different components of visual, auditory and somatic stimuli and are associated with many diseases, such as the inability to feel your own limbs, or recognising faces/objects etc.).
- The primary motor cortex (PMC) is mainly involved with the execution of movements. Populations of neurones in there encode for the direction and amplitude of the movements we make, prior and during the execution.
- The 6 pre-motor cortices, the ventral, medial (supplementary) and dorsal areas are mostly involved with planning our movements. They receive inputs from the cerebellum and basal ganglia, which play very important roles in motor learning (like acquiring new skills) and motor planning. Interestingly, different neurones in the pre-motor areas fire action potentials during execution and are inactive during planning of movements and others vice-versa, while some populations of neurones are active for both planning and execution.
- The prefrontal cortex controls reasoning and decision-making and it is crucial for emotion as well: recall Phineas Gage’s story and how the damage to his prefrontal cortex resulted in a complete change in his personality (article here) as well as how the prefrontal cortex regulates the activity in the hypothalamus and is disrupted in major depressive disorder (article here).
- The limbic system (amygdala, anterior cingulate cortex, hippocampus) , which are located at the subcortical level and behind the frontal lobe, are involved with emotion, fear and the formation of memories, which are so important in our decision making. And these are just the main players, but there are many other areas, including sensory, which contribute to the planning of our actions and the choices we constantly make.
In a rather groundbreaking paper, Libet and colleagues showed that the neural processes leading to the initiation of voluntary movements begin several hundred milliseconds before the reported time of conscious intention to make the movements, as in before the subject is aware of the intention to move. They demonstrated using the readiness-potential (negative electrical potential recorded at the scalp) that brain activity involved in decision-making starts before our brains is conscious of the actions. This is also known as ‘preparatory set”.
Dick Swaab proposed that the unconscious brain areas are active before the conscious ones, in order to enable us to make decisions rapidly and effectively, as the conscious systems require time to process and analyse the pros and cons of every decision. And although it is good to consider the consequences of your actions, there are many other decisions about apparently insignificant things, which we make and need to be fast (like for example, running away from a car you see coming). In a dangerous situation, for example, the parts of the brain involved in consciousness might consider the state of your legs, how capable they are of moving fast at that point, your heart rate, blood pressure, levels of energy needed for that action…Well, by the time your brain finishes analysing all these, you will be most certainly dead.
Another interesting idea Swaab suggested was regarding the reason why we have consciousness of our actions and the things that happen to us in the first place. We need to be conscious of our own experiences so that we learn to avoid negative things in the future and also act upon things that require intervention, such as a wound that needs to be treated. Although the brain seems to be able to plan an action independently of our awareness of it, other brain areas are involved in the execution (as previously mentioned) and the communication between these different parts which fulfil different roles results in consciousness. Exactly why and how evolutionary biology has managed to make us more than just some purely mechanical creatures remains a mystery and still poses many challenges to this field of research, inviting philosophy to have its take on this matter, which many times has proved to be useful.
Swaab also wonders to what extent are criminals, pedophiles, murderers to blame for their bad actions, when it is in fact not them, but their unconsciousness/instincts that dictate them what to do. When considering that people with brain damage resulting in impaired or lack of consciousness (schizophrenia, dementia, multiple sclerosis etc.) sometimes hurt other and are not convicted, you might think that it is right to assume that all criminal acts should be tolerated. However, the difference here is that people not suffering from such disorders are aware of their actions and are capable of stopping them. Although pedophilia is considered a psychiatric disorder, unlike the neurodevelopmental and neurodegenerative ones, it can be controlled by the individual, so that the individual is able to refrain from acting according to his/her instincts. Libet and his team of researchers mention in their study that individuals, although only aware of the intention to make a particular action after the intention has been formed in their brains, are able to “abort the performance” of the action, meaning that they have a conscious “veto”.
They also emphasise the difference between spontaneous, rapidly performed actions, and actions in which a preplanning of the experience occurred (taking into account alternative choices, for instance). This second type of voluntary movements, involving conscious deliberation prior to the act, might actually rely on conscious initiation and control, rather than non-conscious commands. However, this hypothesis has not yet been proved experimentally, in a way the “unconsciousness before consciousness” one has.
So, as it turns out, most of the times we are aware of our brain’s decisions only after they have already been made, and free will seems to be an illusion.
References
Antonio Damasio,1995. Decartes’ Error. Vintage Books, pp. 71-73
Dick Swaab, 2014. We are our brains – From the womb to Alzheimer’s. Penguin Books, pp.326-338
Image by Saya Lohovska. You can find her arts page here.
